Secondary arterial hypertension
Content
Symptomatic arterial hypertension is not an independent disease. This is a consequence of violations in the work of organs and systems that are responsible for the regulation of pressure.
About 15% of cases of hypertension are symptomatic.
The main symptom of this condition is a sudden steady increase in blood pressure, which is difficult to reduce by traditional methods.
In medical circles, another name is popular - secondary arterial hypertension.
Causes and types of symptomatic arterial hypertension

Depending on the diseases or disorders that provoked an increase in pressure, the following types of pathologies are distinguished:
Nephrogenic. In most cases of secondary hypertension, it was caused by acquired or inherited pathologies of the kidneys or nearby arteries. Moreover, in the primary stages of the disease, they cannot lead to an increase in pressure. More often this condition is characteristic of severe forms. Pyelonephritis (an infection in the renal pelvis) and glomerulonephritis (a consequence of frequent tonsillitis) are the most common factors leading to an increase in pressure. Tumors, injuries, compression of the kidneys, developmental anomalies, urolithiasis and other diseases are no less dangerous.
Endocrine. This type of hypertension develops due to disorders in the endocrine system and pathologies of the glands:
- thyrotoxicosis (excessive release of the hormone thyroxin into the blood, which leads to an increase in systolic pressure with a stable diastolic pressure);
- pheochromocytoma (a neoplasm in the adrenal glands, the pressure rises abruptly or constantly high);
- Conn's syndrome (the production of the hormone aldosterone increases, which prevents the excretion of sodium from the body, resulting in its excess in the blood);
- Itsenko-Cushing's syndrome (characterized by a distortion of the proportions of the body, when the torso and face get better, and the limbs remain as they were); menopause (hormonal changes that occur at the end of reproductive function can cause an increase in pressure).
Neurogenic. The basis for their appearance are disorders of the central nervous system (tumors, brain injuries, ischemia, encephalitis). In addition to increased pressure, the patient complains of intense headaches, profuse salivation, convulsions, tachycardia.
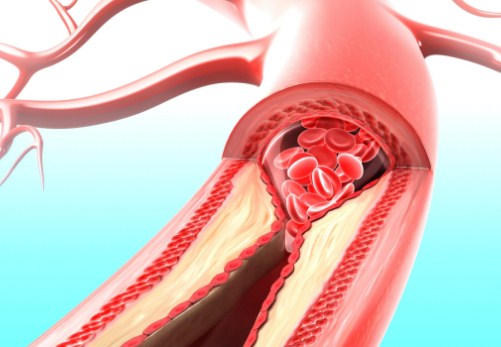
Hemodynamic. For this type of symptomatic hypertension, an increase in the upper (systolic) index is inherent. As a rule, the cause is the pathology of important arteries and the heart (bradycardia, atherosclerosis, mitral valve disease, congenital narrowing of the aorta, heart failure).
Medicinal. Symptomatic hypertension can occur while taking drugs that increase blood pressure (adrenergic agonists) or affect hormonal regulation (contraceptives, glucocorticoids).
Also, symptomatic arterial hypertension develops as a result of chemical poisoning (lead, cadmium or thallium), chronic lung diseases, an excessive number of red blood cells (polycythemia).
Depending on the severity of the course, symptomatic hypertension is divided into the following forms:
- Transient. The pressure rises periodically for several hours or days and normalizes on its own. This is the easiest stage of hypertension, which is important to identify and eliminate in time.
- Labile. The indicators of the tonometer increase after suffering stress or physical exertion. Differs in resistance, to reduce it requires treatment. There may be mild left ventricular hypertrophy and slight vasospasm on the inside of the eyeball.
- stable. The pressure is stable and serious therapy with constant medication maintenance is needed to normalize it. There is a strong increase in the muscle tissue of the left ventricle and deformation of the eye vessels.
- Malignant. The most dangerous form of hypertension with a high risk of life-threatening complications. The pressure rises rapidly, the diastolic index reaches 130 mm Hg. Art.
Distinguishing features of symptomatic hypertension
If hypertension is easy to identify with a tonometer, then distinguishing its nature is not an easy task. Often, this requires careful studies of the whole organism (biochemical, radiographic, radioisotope, and others), some of which are quite painful.
Therefore, through long-term observations, it was possible to identify special signs by which symptomatic arterial hypertension can be suspected:
- Sudden development and rapid progression of hypertension.
- Sustained pressure that is rarely reduced by traditional means.
- Sympathetic-adrenal crises (panic attacks).
- The age of the patient is very young (up to 20 years) or, conversely, quite advanced (60 and older).
- Rise in diastolic pressure.
It is impossible to establish a correct diagnosis on your own, only an experienced doctor will be able to identify and distinguish between symptomatic and primary hypertension.
Therefore, if there are signs of increased pressure, you should seek medical help.
Diagnosis of pathology
Diagnosis of symptomatic hypertension is carried out depending on the etymology and includes 3 stages:
- The study of past illnesses.
- Identification of patient complaints.
- Appointment of the necessary studies and analyzes.
The patient's previous or chronic illnesses make it possible to formulate a diagnostic direction.
Nephrogenic hypertension. The patient's complaints about swelling of the extremities, frequent urination, changes in the physical characteristics of urine, and abdominal pain make it possible to associate an increase in pressure with pathological processes in the kidneys. If a high temperature is observed, this indicates a urinary tract infection or the presence of a tumor. Additionally, with the help of palpation, the doctor detects hydronephrosis, hypernephroma or polycystic kidney disease. Based on the current data, it is already possible to formulate a preliminary diagnosis. The next step will be the referral to the studies that are needed for the final conclusion. In addition to general tests for hypertensive patients, the following procedures can be prescribed:
- CT and ultrasound of the kidneys;
- total and separate study of the work of the kidneys;
- contrast angiography;
- detection of renin and angiotensin in the blood;
- quantitative assessment of the degree of bacteriouria;
- daily concentration of protein in the urine.
Often, for many years, kidney pathologies proceed secretly, and it is quite difficult to identify them. Nephrogenic hypertension is more typical for severe forms of renal disease. 
endocrine hypertension. At the stage of preliminary examination, the patient complains of hypertensive crises, which are accompanied by palpitations, pallor of the skin, sweating, muscle tremors, and headache. The combination of these symptoms makes it possible to suspect pheochromoblastoma in a patient. Pheochromocytoma is characterized by the presence of syncope and persistently high blood pressure. If the patient voices complaints about frequent urination at night, increased fatigue, general weakness, thirst, this may indicate Conn's syndrome. When high fever and abdominal pain are added to the listed signs, he most likely has adenocarcinoma of the adrenal gland. Increased body weight, violations of the sexual sphere, along with hypertension, signals Itsenko-Cushing's disease. It is possible to confirm such a diagnosis if there is still itching of the skin, polyuria and thirst in the patient. After conducting general studies in endocrine hypertension, the following changes are likely:
- persistent alkaline urine reaction (due to the high concentration of potassium);
- hyperglycemia or hypokalemia;
- leukocytosis and erythrocytosis.
Further more accurate studies are carried out according to the doctor's prescription, depending on the alleged diagnosis.
hemodynamic hypertension. Almost all cases of increased pressure in this type of hypertension occur against the background of pathologies of the heart and large vessels that disrupt systemic blood flow. Basically, the systolic index increases. At the very beginning, the doctor receives information from the patient about the presence of atherosclerosis and its manifestations, the features of increased pressure (time of day, sensations), the presence of heart failure or other diseases associated with large arteries or the heart, the effectiveness of drug therapy. Often the cause of hemodynamic hypertension is atherosclerosis of varying severity. Patients complain:
- to a feeling of coldness in the extremities;
- the pulse in the arteries of the arms and legs is reduced.
 If a pronounced systolic murmur is heard during auscultation of the heart, this may indicate atherosclerosis of the aorta. A doctor will suspect the diagnosis of "coarctation of the aorta" when blood pressure is elevated in the upper extremities and simultaneously reduced in the lower ones. At the same time, during the examination, an intense pulsation of the intercostal arteries and a weakening of the pulse in the peripheral ones are revealed. The clinical picture is confirmed by auscultatory examination of heart murmurs. With atherosclerosis, an increased level of cholesterol and triglycerides is found in the blood (a study of the lipid spectrum). After electro- and echocardiographic, X-ray examination of the heart, its defects are revealed. Patients with coarctation of the aorta have an angiogram before surgery to determine the location and size of the affected area.
If a pronounced systolic murmur is heard during auscultation of the heart, this may indicate atherosclerosis of the aorta. A doctor will suspect the diagnosis of "coarctation of the aorta" when blood pressure is elevated in the upper extremities and simultaneously reduced in the lower ones. At the same time, during the examination, an intense pulsation of the intercostal arteries and a weakening of the pulse in the peripheral ones are revealed. The clinical picture is confirmed by auscultatory examination of heart murmurs. With atherosclerosis, an increased level of cholesterol and triglycerides is found in the blood (a study of the lipid spectrum). After electro- and echocardiographic, X-ray examination of the heart, its defects are revealed. Patients with coarctation of the aorta have an angiogram before surgery to determine the location and size of the affected area.
 neurogenic hypertension. Associated with malfunctions of the nervous system. Along with complaints of high blood pressure, the patient indicates severe headaches and cases of epilepsy. Previously received injuries, encephalitis, arachnoiditis, concussions are likely. At the initial stages of CNS diseases, characteristic symptoms may be absent. Only with a prolonged course, deviations in behavior, impaired coordination of movements, and the functioning of the sense organs are noticeable. In the elderly, symptoms of CNS disease are easily confused with cerebral atherosclerosis. The most important task with the help of research is to prove or disprove the presence of a brain tumor. According to medical indications, the following diagnostic methods are prescribed:
neurogenic hypertension. Associated with malfunctions of the nervous system. Along with complaints of high blood pressure, the patient indicates severe headaches and cases of epilepsy. Previously received injuries, encephalitis, arachnoiditis, concussions are likely. At the initial stages of CNS diseases, characteristic symptoms may be absent. Only with a prolonged course, deviations in behavior, impaired coordination of movements, and the functioning of the sense organs are noticeable. In the elderly, symptoms of CNS disease are easily confused with cerebral atherosclerosis. The most important task with the help of research is to prove or disprove the presence of a brain tumor. According to medical indications, the following diagnostic methods are prescribed:
- electroencephalography;
- Ultrasound and CT;
- x-ray of the skull (allows to identify large tumors);
- rheoencephalography.
Secondary arterial hypertension can be both the main symptom of the disease and a secondary one (rarely noted in the diagnosis).
Treatment of secondary arterial hypertension
Therapy of secondary hypertension is based on the elimination of the causes that led to the disease state.
Surgery is necessary if the increase in blood pressure is caused by:
- vascular pathology;
- pheochromocytoma;
- coarctation of the aorta;
- hypernephroid kidney cancer.
In the case of pituitary adenoma, treatment is carried out with the help of a laser, radio and X-ray therapy, in some situations, surgery is also performed.
A positive result in the elimination of secondary hypertension is given by treatment with antihypertensive drugs. More often than not, several drugs with different effects are prescribed. They have a large number of contraindications and side effects, so treatment with synthetic drugs should only take place under the supervision of an experienced physician. If antihypertensive therapy is ineffective, peripheral vasodilators and adrenoblockers are used.
Symptomatic hypertension caused by kidney damage involves the use of diuretics (diuretic drugs) in combination with ACE inhibitors.
More often, combined drug treatment gives a positive result if the patient suffers from stable (in particular, diastolic) hypertension of any origin.
 In the treatment of the disease, the age characteristics of the patient should be taken into account. Elderly people with long-term and stable hypertension should not reduce pressure too sharply. This often leads to deterioration of coronary, cerebral and renal blood flow.
In the treatment of the disease, the age characteristics of the patient should be taken into account. Elderly people with long-term and stable hypertension should not reduce pressure too sharply. This often leads to deterioration of coronary, cerebral and renal blood flow.
In some cases, it is acceptable to use a small amount of cordiamine and caffeine to tone the vessels of the brain and stimulate nerve impulses. It is better to apply them in the morning when the pressure is the lowest.
Preventive actions
 The main goal in this case is to reduce the risk of developing diseases that are accompanied by an increase in pressure. Timely treatment of chronic diseases and acute infections is also important.
The main goal in this case is to reduce the risk of developing diseases that are accompanied by an increase in pressure. Timely treatment of chronic diseases and acute infections is also important.
Systematic physical training is especially useful. Indeed, in a person who leads a sedentary lifestyle, metabolism worsens, muscles weaken, blood stagnation appears in the pelvic organs and limbs. As a result, the risk of cardiovascular disease increases.
One of the first recommendations for the prevention of high blood pressure and other diseases is the optimization of work and rest.
Negatively affect health:
- difficult working conditions;
- no vacation;
- night shifts;
- stressful situations.
Overwork reduces the body's defenses, and it is more exposed to pathogenic factors.
In order not to lose your ability to work at all, you should:
- fully rest;
- exercise;
- spend a lot of time outdoors;
- give up bad habits (the risk of hypertension in drinkers is 3 times higher).
/div>