Prognosis for acute transmural infarction of the anterior or inferior wall of the myocardium
Content
Transmural myocardial infarction is a dangerous consequence of coronary heart disease (CHD). With this pathology, the lack of blood supply leads to necrosis of a part of an organ. Currently, the most common cause of death is cardiovascular disease. In nine out of ten cases, a person dies due to an acute heart attack of the heart muscle. If first aid is not provided on time, then severe complications and inevitable death occur, the probability of which reaches 35%, which is a rather high indicator. At the age of 40-60, males are affected by this disease several times more often than women. This is a consequence of the earlier development of atherosclerosis in men. It is useful to know the prerequisites for the development of the disease, the symptoms, remember the emergency measures when it occurs, and provide recovery options.
Description

- the outer layer is called the epicardium;
- the middle layer is the mural layer (myocardium);
- the inner layer is called the endocardium.
The epicardium and endocardium, which consist of connective tissue, are tightly connected by the myocardium. The epicardium is weakly involved in the process of contraction of the heart muscle. The endocardium is largely involved in the contraction process. He is the first to experience ischemic lesions. The next to be affected is the myocardium. The epicardium is the last to be damaged.
A heart attack can be:- intramural, when lesions occur in only one layer;
- non-transmural, in which not all layers of the membrane are affected;
- subendocardial, when the focus is localized in the upper layers of the myocardium;
- transmural (through), in which necrotic foci occur in all layers (the most dangerous condition).
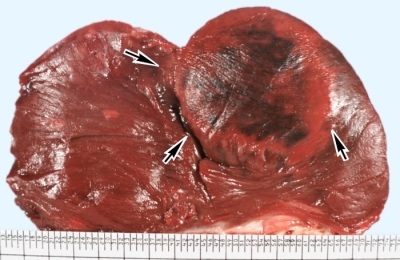
The transverse size of lesions in transmural infarction (TI) can be 2-8 cm. The lesion can be small-focal and large-focal (extensive).
The most severe form of pathology is acute TI, in which all layers are affected by necrosis. Up to 20% of patients who have this condition die within one month. When recovering from a heart attack, connective tissue replaces damaged areas, which leads to the development of post-infarction cardiosclerosis.
Physicians sometimes refer to TIs as "penetrating" (Q-type). Its features are the rapid dynamics of development, a large number of dead cells.
Depending on the location of the focus, acute transmural infarction is isolated, passing with damage to the anterior or lower wall of the myocardium. Anterior TI is more often observed, the lower variant is usually more severe and more difficult to diagnose. In 33% of cases, necrosis affects the atria, in one case out of five lesions appear in the right ventricle.
Prerequisites for pathology
 A heart attack is a consequence of a lack of incoming blood to feed an organ (or part of it). If nutrients and oxygen are not supplied in sufficient quantities, then the cells begin to die (necrotic changes occur). TI is also a consequence of an insufficient supply of blood to the heart muscle.
A heart attack is a consequence of a lack of incoming blood to feed an organ (or part of it). If nutrients and oxygen are not supplied in sufficient quantities, then the cells begin to die (necrotic changes occur). TI is also a consequence of an insufficient supply of blood to the heart muscle.
Pathological changes in the blood supply appear with atherosclerosis due to the blockage of the lumen by plaques. This leads to a lack of oxygen and essential substances, which is not very noticeable in the absence of exercise.
With physical or psycho-emotional overload, the speed of blood flow increases, and a turbulent eddy occurs near the plaque. The inner surface of the artery is damaged, which contributes to the formation of a blood clot, further exacerbating problems with blood flow. With a lack of oxygen, the cells of all layers of the shell of the heart begin to die.
The supply of the heart with blood has some features:- for the full functioning of the myocardium, three times more oxygen is required than for a normal muscle with the same mass;
- with a lack of oxygen, a rapid expansion of the supply vessels occurs;
- with insufficient blood supply, the branched network of collateral vessels is activated, which under normal conditions are “in reserve” and are not actively used.
However, the possibilities of compensation mechanisms are limited.
Acute circulatory disorders of the myocardium may be due to:- Thrombosis or vascular embolism with complete blockage of the bloodstream. Certain types of poisoning, thrombophlebitis, anemia, diabetes mellitus contribute to the formation of blood clots.
- A sharp increase in the need for oxygen, if the vessels cannot provide it in the required amount. This situation is realized with high physical or psycho-emotional stress, with a hypertensive crisis or tachycardia.
- Stenosis (a significant decrease in the lumen) of the supply vessels.
 There is an interrelationship between these mechanisms.
There is an interrelationship between these mechanisms.
Violation of blood supply to the myocardium for 15-20 minutes leads to the onset of irreversible necrotic changes in muscle tissue.
The risk factors for TI are as follows:- age over 45 years;
- hereditary tendency to this type of pathology;
- high cholesterol;
- excess body weight;
- smoking;
- alcohol abuse;
- hypodynamia;
- improper diet (excess of animal fats);
- frequent stress and emotional overload;
- certain diseases (diabetes mellitus, coronary artery disease, hypertension).
Symptoms
Symptoms in TI are different and are determined by the nature of the course of the pathology.
However, in most cases, the following symptoms are characteristic:- high heart rate (tachycardia);
- prolonged pain of variable severity that does not go away for many hours (usually up to one day);
- severe pain of a compressive nature, radiating to the left forearm (sometimes to other parts of the body);
- feeling of "fading" of the heart;
- systolic murmurs;
- release of cold sweat;
- excessive excitement, which is accompanied by a fear of death;
- pronounced psychosomatic reactions;
- pallor and cyanosis of the skin and mucous membranes;
- weak pulse, low blood pressure;
- speech disorders and loss of consciousness are possible;
- shortness of breath, suffocation, which resembles asthma attacks.
In the case of acute TI, the same manifestations are found as in a normal heart attack, but in a more severe form. The severity of the symptoms is due to the fact that with TI, a significant part of the heart muscle is suddenly completely excluded from the blood circulation.
 On the second day the temperature rises to 38-39 o C and does not decrease during the week. Arrhythmias are observed in 43% of cases.
On the second day the temperature rises to 38-39 o C and does not decrease during the week. Arrhythmias are observed in 43% of cases.
- Anginal. A person feels tearing pains in the chest, radiating to the arms, as well as to the area of the entire chest. Characterized by dizziness, weakness. The duration of the attack is from 15 minutes to 24 hours.
- gastralgic. A sharp pain in the epigastrium is typical, often there is vomiting that does not bring relief. Such manifestations are observed in one case out of twenty. Quite often the preliminary diagnosis is erroneous.
- Asthmatic. There may be no pain. Characterized by suffocation, rapidly occurring pulmonary edema.
- Cerebral. This very rare variety is similar to a stroke, often without pain.
Diagnostics
TI is the most dangerous condition, therefore, if this pathology is suspected, help is required immediately.
Prior to the arrival of the doctor, the following measures should be taken:- immediately call an ambulance;
- the victim should lie (half-sitting) with legs slightly bent at the knees in a position close to horizontal;
- you need to loosen tight clothes, take off your tie;
- the victim should take one tablet of nitroglycerin. If the pain does not stop, then after five minutes the second tablet is taken (no need to give more than three tablets of nitroglycerin), you must first measure the pressure (if the readings are less than 90 mm Hg, nitroglycerin should not be given);
- the victim must chew tablets of acetylsalicylic acid (at a dose of 300 mg);
- if the victim suffers from shortness of breath, wheezing is heard in the lungs, then he should be in a sitting position with a pillow placed under his back;
- if the ambulance is delayed for a long time, then it is necessary to quickly, but carefully (avoiding sudden movements) deliver the victim to the nearest hospital;
- if the victim has no consciousness, pulse, respiratory instability, a heart massage (indirect) and (or) artificial respiration is done.
 These simple actions can save a person's life until the doctors arrive.
These simple actions can save a person's life until the doctors arrive.
To diagnose TI, an electrocardiogram (ECG) is measured. An experienced cardiologist, based on the cardiogram, establishes the localization of the affected area, approximately determines the area of the lesion, and distinguishes TI from other cardiopathologies accompanied by necrosis.
In addition, according to the cardiogram, the prescription of necrotic changes is established, conclusions are drawn about the depth and prevalence of lesions. It is important to identify areas of damage around the focus, where the changes are still reversible. The cardiogram depends on the stage of development of the pathology, it changes with the restoration of cells and scarring.
Important information is provided by a blood test - for example, about the area of the affected area. After TI, the number of leukocytes increases, which remains at a high level for 14 days. When the leukocytosis passes, the ESR will increase.
Methods of treatment, recovery and prognosis
Treatment for TI is aimed at:
- elimination of pain and psychological disorders;
- fight against the formation of blood clots;
- normalization of the rhythm of contractions;
- reduction of the area of ischemia;
- ensuring the beginning of scarring of the area of necrosis;
- restoration of blood supply to all organs;
- prevention of complications and recurrence of the disease.
 Narcotic drugs (for example, morphine) are used to overcome severe pain, and tranquilizers are used for mental correction. In thrombolytic therapy, the use of fibrinolysin, alteptase, and heparin is practiced. To combat arrhythmias, drugs that block beta-adrenergic receptors, as well as peripheral vasodilators (for example, nitroglycerin), are used. In order to form a dense scar, anabolic hormones and restorative agents are prescribed. To prevent repeated attacks, acetylsalicylic acid, beta-blockers, nitrate drugs, drugs with inhibitory properties are used. Maintenance therapy is often lifelong.
Narcotic drugs (for example, morphine) are used to overcome severe pain, and tranquilizers are used for mental correction. In thrombolytic therapy, the use of fibrinolysin, alteptase, and heparin is practiced. To combat arrhythmias, drugs that block beta-adrenergic receptors, as well as peripheral vasodilators (for example, nitroglycerin), are used. In order to form a dense scar, anabolic hormones and restorative agents are prescribed. To prevent repeated attacks, acetylsalicylic acid, beta-blockers, nitrate drugs, drugs with inhibitory properties are used. Maintenance therapy is often lifelong.
Proper nutrition is essential for recovery. It is necessary to eat rough, easily digestible food. It is necessary to eat in small portions, but often (5-6 times a day). At the first stage, it is useful to use cereals, dried fruits, juices, kefir. Do not interfere with products that help empty the intestines (dried apricots, beets). Subsequently, other foods are included in the diet, but fatty foods rich in cholesterol must be abandoned for life.
A person should gradually return to physical activity. At the first stage, it is necessary to prevent congestion in the lungs, muscle atrophy, and other consequences of prolonged exposure to static positions.
Preventive measures are to exclude provoking factors.
 For this you should:
For this you should:
- Eliminate smoking from your life
- eat right (low cholesterol diet, limit salt intake);
- lose weight;
- control blood pressure;
- try to eliminate stress and physical overload.
- thromboembolism;
- ventricular fibrillation;
- paralysis of the limbs;
- problems with speech function;
- pulmonary edema;
- failure of internal organs;
- heart break.
The prognostic assessment is determined by the size of the foci. If more than 50% of the heart muscle is affected, then there is no alternative to death. If the area of the lesion is small, then the probability of death due to complications remains.
When the acute period passes without significant complications, the prognostic assessment remains conditionally unfavorable due to the irreversible nature of the lesions. In the case of a favorable outcome, the patient expects a long recovery.