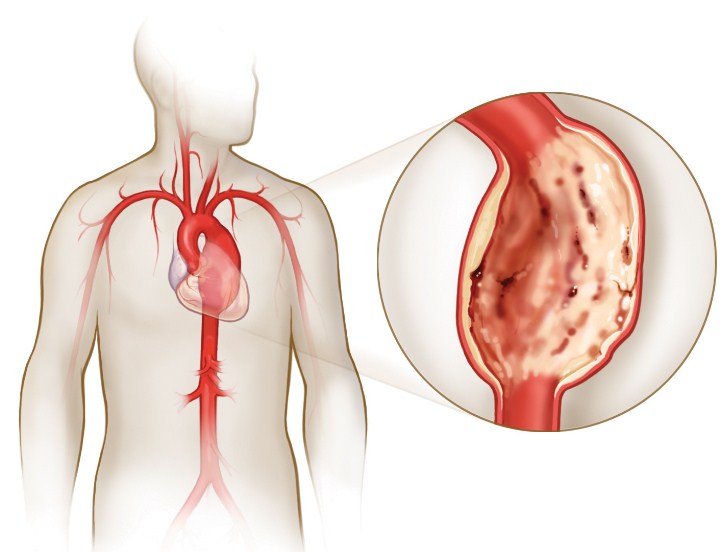
What is a heart aneurysm?
Sometimes irreversible consequences are brought with it by an aneurysm of the heart in its clinical development.
A pathological defect in any small chamber of the main muscular organ in the form of thinning of the myocardium or its rupture triggers an extensive symptom complex. Cardiac asthma, shortness of breath, thromboembolism of large vessels can develop suddenly against the background of the pathogenesis of the aneurysm, so that there is a limited time for treatment. Most often, a surgical operation is necessary to resolve the condition of such patients.
The essence of pathogenesis

Clinically, cardiac aneurysms pose a constant risk of death. Prevention of such a disease is mandatory after a heart attack.
For a long time, cardiac aneurysms remained little studied, since the diagnostic equipment of the last century could not detect the smallest defects in the muscular wall of the heart:
- It was possible to consider large defects, and over time, clinical specialists began to draw analogies to clarify the diagnosis.
- Today, ultrasound reflects the picture of an aneurysm of the heart in the form of clarification of the boundaries of the myocardium.
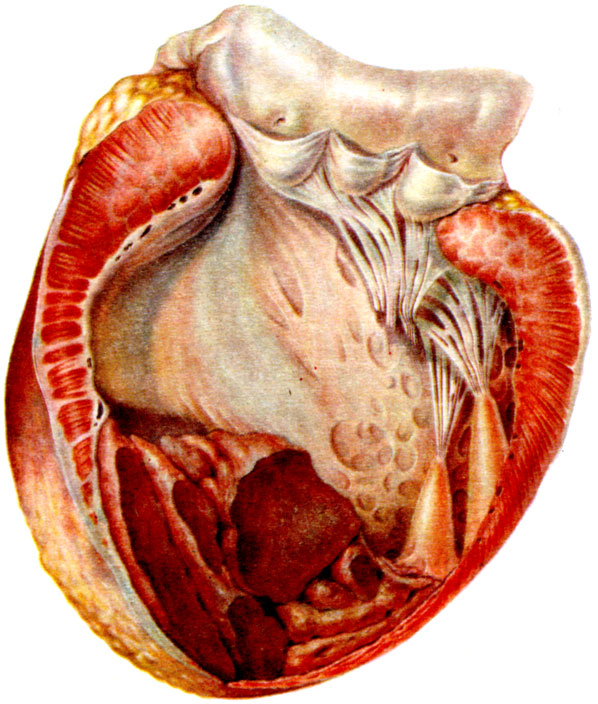
 Statistical data in cardiology revealed a pattern of heart aneurysm and myocardial infarction in history. This pathology occurs more often in men of mature and advanced age. The predominant localization of aneurysms was also revealed, which most often appear in the left ventricle, a little less often in the cardiac septum and the right heart. Clinically significant aneurysm of the heart is more than one centimeter, but they reach a diameter of twenty centimeters.
Statistical data in cardiology revealed a pattern of heart aneurysm and myocardial infarction in history. This pathology occurs more often in men of mature and advanced age. The predominant localization of aneurysms was also revealed, which most often appear in the left ventricle, a little less often in the cardiac septum and the right heart. Clinically significant aneurysm of the heart is more than one centimeter, but they reach a diameter of twenty centimeters.
This circulatory disorder has two significant types for the rate of development of acute conditions:
- Akinesia is the complete cessation of myocardial contractility.
- Dyskinesia is a borderline condition of the defect, when systole is accompanied by retraction of the aneurysm, and diastole is accompanied by its bulging.
Clinically significant etiology
The main reasons for the development of aneurysms are clinically significant in view of the fact that they determine the main preventive directions for these conditions.
In the etiology of a heart aneurysm, it usually happens:
- Myocardial infarction makes up the vast majority of predisposing causes for dissection of the heart wall. Data show that 95% percent of patients suffered transmural infarction, ischemic damage to the apex or anterior wall of the left ventricle. The pathogenesis of a heart attack determines the dysfunction of the cardiac muscle, which tends to compensate for its condition by developing an additional chamber in the form of an aneurysm. But usually it does not make up for the lost function, it quickly becomes thinner and tears. But such a muscular defect in the heart can exist for a long time, until complete wear occurs.
- Heart aneurysms also develop with an increased load on the organ with progressive arterial hypertension, infectious and somatic heart diseases, and other causes associated with errors in a healthy lifestyle. The latter directly determine atherosclerotic damage to the heart and large vessels.
- Aneurysm can also be congenital. Then it is associated with other defects affecting the valves of the heart, septa between the departments of the organ, and forms anomalies in the localization of blood vessels.
- Injuries to the heart and chest are separate causes of aneurysms. Closed or open injuries of organs, as well as equivalent surgical interventions, determine the dysfunctional work of the heart, which thins and wears out the myocardium with the formation of protrusions.
Since a heart attack becomes a frequent trigger for the development of an aneurysm of the heart, the classification of the disorder was formed based on the time of its development from the moment of ischemia:
- An acute aneurysm can develop within a week of an ischemic attack. In this case, the necrotic myocardium acts as a material for the formation of a fighting cavity.
- The timing of the development of subacute pathology is limited to eight weeks. The cavity is already formed from the endocardium, in which there are islands of fibroblasts and other connective tissue elements that have come to the site of the destroyed myocardial tissue.
- It takes more than two months for a chronic aneurysm to form. The nature of such a formation becomes more complicated, the aneurysm already has three layers, but thus it does not acquire strength. Occasionally, the overlap of the endocardial, intramural, and epicardial layers may not exceed two layers in total. Endocarditis is usually represented by hyalized tissue, and the aneurysm cavity may even contain a thrombus. A fibrin clot can be located near the wall, or it can even occupy the entire volume of the aneurysm, which makes the condition potentially dangerous in terms of thromboembolic complications.
An aneurysmal protrusion is usually an independent formation, sometimes there may be several chambers in it. Rare are cases when a patient has several aneurysms located nearby or remotely.
The contours of the pathological defect can be very non-standard. Ultrasound diagnosticians distinguish mushroom-shaped, saccular aneurysms, flat and diffuse formations.
Clinical manifestations
Since this pathology is directly related to the heart, for convenience, the symptoms are divided into two groups:
Cardiac:
- failures of the heart rhythm, its acceleration or slowdown. The patient himself can feel interruptions in the work of the organ, but more often this is reflected in the cardiogram. Fibrillations and extrasystoles are possible, which are registered or not;
- cardiac asthma followed by pulmonary edema gives symptoms of shortness of breath and shortness of breath. Edema and pastosity may develop.
Extracardiac symptoms are also extensive:
- syncopal manifestations in the form of dizziness, cramping headache, sparks from the eyes, fainting can develop quite quickly;
- heart aneurysms are also accompanied by sweating, which is easily confused with intoxication syndrome;
- in this condition, ascites may increase, the liver and spleen may increase irrationally.
Occlusive phenomena in the extremities, arterial basin of the kidneys and brain help to suspect thrombotic disorders. This manifestation of an aneurysm is sometimes complicated by gangrenes, strokes, repeated heart attacks, which are quite problematic to treat.
Chronic aneurysms of the heart rarely rupture with blood effusion and associated complications.
Fatal are acute pathologies that occur almost immediately after an episode of myocardial ischemia.
A sufficiently pronounced clinic of the pathological condition allows a disorder to be suspected:
- The patient turns pale, the extremities become cold.
- Cardiac tamponade due to the increasing volume of outflowing blood gives a clinically pronounced overflow of the veins of the neck.
- The patient may breathe shallowly and noisily, faint.
ECG diagnostics helps to quickly recognize an aneurysm. The cardiogram shows signs of a massive infarction, which freezes in contrast to transient ischemia. An echocardiogram is also informative, which allows you to determine the volume of the cavity that formed the aneurysm of the heart. With its help, thrombotic accumulations are also recognized as occlusion foci.
 The radiograph allows visualizing the presence of cardiomegaly, which corresponds to organ hypertrophy as a consequence of the myocardium. The use of the method with contrast, as well as magnetic resonance imaging, clearly localize the aneurysm, determine its volume and the likelihood of tearing.
The radiograph allows visualizing the presence of cardiomegaly, which corresponds to organ hypertrophy as a consequence of the myocardium. The use of the method with contrast, as well as magnetic resonance imaging, clearly localize the aneurysm, determine its volume and the likelihood of tearing.
Difficulties in a differentiated diagnosis arise when a cardiac aneurysm is similar to pericardial cysts, clinically comparable to symptoms in mitral valve disease. A similar clinic is also given by malignant tumors of the mediastinum with invasive growth.
Cardiac aneurysms are treated surgically in most cases when surgery is timely. Acute and subacute formations are operated on for the purpose of suturing defects to prevent their rupture. Chronic aneurysms are compensated by various methods to avoid thrombotic and occlusive complications.