Mitral regurgitation 1 and 2 degrees
Content
Is mitral valve regurgitation life-threatening or not? Perhaps, this will primarily excite a person who has heard such a diagnosis, because we are talking about the heart, the main organ of the human body, without which it is impossible to live.
It depends on the degree of damage to the valve leaflets, on the cause that caused regurgitation and on how the pathology develops.
In order to answer this question, it is necessary to consider what physiological changes occur in this organ and how they affect health.
What happens in the heart during the development of regurgitation

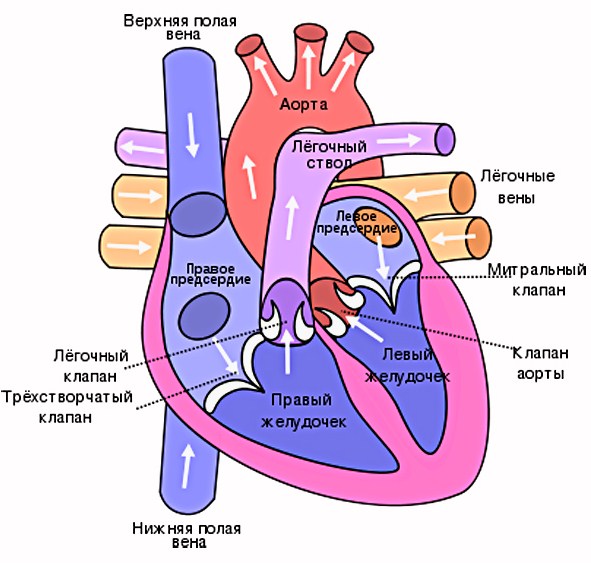
Probably, many still remember from school that a person consists of 2 atria and 2 ventricles, the work of which can be schematically described as follows:
- Blood from the vessels enters the atrium (in the right - venous, in the left - arterial).
- Filled with blood, the atria contract, pushing their contents into the ventricles, while the valves open (tricuspid on the right, mitral on the left).
- After all the fluid has flowed into the ventricles, the valves close tightly, preventing backflow.
- After the valves close, a powerful contraction of the ventricles occurs, blood rushes through the arteries.
The left side of the heart works with a higher load, because it supplies blood to all organs and tissues of the body. This is what happens normally.
In doing so, the following happens:
- To accommodate the blood that has flowed from the ventricle and entered through the veins, the atrial chamber gradually increases. At the same time, due to the fact that the atrial cavity is partially filled at the moment of relaxation, the blood flow in the pulmonary veins worsens, leading to stagnation in the pulmonary circulation.
- The flow of increased volume of blood flow from the atrium into the ventricular cavity gradually leads to its increase.
The degree of health risk in this pathology depends on the size of regurgitation and how it develops.
The size of the divergence of the leaflets when the valve is closed
According to the size of the valve gap remaining after the closure of the valves, the following degrees of development of the pathology are distinguished:
- I degree. The gap after closing the valves is insignificant, and patients do not present any complaints. The presence of regurgitation of the 1st degree is detected only during a medical examination, when during auscultation a heart murmur is heard in the apical region and a weakening of the 1st tone. Some people have physiological regurgitation, when the valve leaflets are healthy, but at the time of contraction of the ventricle, a small amount of blood passes.
- II degree. With it, the return of blood volume can reach the middle of the atrial chamber. If the returned volume is a quarter or more, then the patient, in addition to the occurrence of characteristic noises, may experience signs of stagnation in the pulmonary circulation.
- III degree. The flowing fluid reaches almost the posterior wall of the atrium, causing its overload and provoking stagnant processes in the pulmonary veins. Gradually overload occurs in the right half of the heart. Patients with III degree of regurgitation complain of fatigue, shortness of breath, in some cases asthma attacks are possible.
- IV degree. Congestion becomes more pronounced, patients complain of shortness of breath, pain in the heart, severe fatigue. Due to congestion in the pulmonary circulation, a person develops hypertrophy of the right cardiac sections. In severe cases, cardiac asthma and pulmonary edema may occur.
At the I degree of regurgitant casting, treatment is not required, such patients are only under medical supervision. Grade II is treated conservatively, drugs are prescribed to relieve the symptoms that have arisen and to treat the underlying disease that caused valve deformity or prolapse.
The indication for surgical intervention is the non-closure of the valves up to 45 mm and the return of more than 60% of the volume at the time of ventricular contraction.
Diagnostic methods
In order to identify the presence of pathology and the degree of its development, the following methods are used:
- X-ray. An x-ray will show enlargement of the left side of the heart. With advanced pathologies, an increase in all departments of the organ is possible.
- ECG. This method is not informative. Only in the case when the posterior papillary muscle of the myocardium is affected, negative T waves are recorded on the electrocardiogram in II and III leads, moderate tachycardia is noted.
- Echocardiography. The study allows you to determine the size of the valvular gap at the time of closure of the valves, the amount of reverse reflux and the cause of the violation (prolapse, rupture of the valve muscles or destructive changes).
- Transesophageal echocardiography. It is used infrequently, mainly in severe cases. Allows you to determine whether there is myocardial ischemia, the presence of fibrosis or calcification in the valve tissue.
- Dopplerography. Study of the magnitude and speed of blood flow. Gives a complete picture of blood exchange in the entire vascular bed.
How the disease develops
Pathology, depending on the causes that caused it, can develop:
- acute;
- chronically.
Acute process development
In acute valvular insufficiency, symptoms increase rapidly.
A person develops:
- stagnation of blood first in a small, and then in a large circle of blood circulation;
- pulmonary edema, often bilateral;
- insufficiency of both ventricles;
- cardiogenic shock.
Such patients need urgent hospitalization and resuscitation. With untimely assistance, a fatal outcome is possible.
Chronic course of the disease
In this case, the pathology develops gradually, at the initial stage it can be asymptomatic or accompanied by a slight pain syndrome and shortness of breath with little physical exertion.
With the further development of the disease:
- cardiac decompensation occurs;
- stagnation of pulmonary blood flow develops;
- there are disturbances in the work of the right atrium, and then the ventricle.
If the disease was not diagnosed in a timely manner, the person did not start treatment, then in the future the heart increases in size and is no longer able to provide a full blood supply to organs and tissues. Insufficiency of a large circle of blood circulation develops.
Is mitral valve regurgitation dangerous?
Timely detected and treated disease allows a person to avoid complications for many years and lead a full-fledged lifestyle.
As medical statistics show, the progression of the development of pathology occurs only in 10% of all identified cases.