Indications for coronary artery bypass surgery and patient reviews
Content
The lack of blood supply caused by narrowing of the arteries of the heart can lead to coronary insufficiency, and in the case of complete occlusion, to myocardial infarction. In a significant proportion of patients, the result of drug therapy for this condition is insufficient, therefore, invasive methods of treatment are resorted to to restore normal blood flow. Heart bypass surgery: what is this operation and what is its result?
The essence of the method and indications for surgery

Coronary artery bypass grafting is a method of restoring blood flow by creating an anastomosis (shunt) that bypasses the area with obstruction. Most often, a vein from the lower limb of the patient, usually not affected by atherosclerosis, is used for this, which connects the aorta and the coronary artery below the site of the lesion. However, the functionality of venous grafts deteriorates significantly already five years after the operation: the tone of the vascular walls is disturbed, blood flow slows down, and thrombosis may develop. The best result can be achieved by using as a shunt the internal arteries of the chest that are close in diameter (mammary or bimammary shunting) and the arteries of the forearm, which can withstand very high blood pressure in the aorta.
The choice of vessel is one of the key factors affecting the outcome of the operation in the long term. A year after surgery, up to 20% of venous bypasses are closed, and ten years later, about 50% of them require replacement, while up to 90% of arterial grafts remain patency.
There are a number of indications for the operation.
These include:- significant arterial stenosis caused by atherosclerotic lesions;
- multiple blockage of arteries;
- damage to the left coronary artery;
- pathology of the heart valves;
- aneurysms of the arterial wall;
- inability to install a coronary stent;
- reduced pumping function of the heart;
- sudden closure of the lumen of the artery with the development of thrombosis during the operation of stenting (emergency shunting);
- severe angina.
A recent stroke, the presence of severe internal diseases, incl. incurable, high obesity, high risk of death and development of severe complications are contraindications to coronary artery bypass grafting.
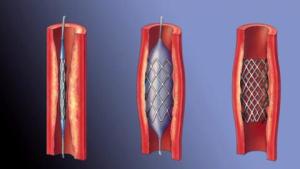
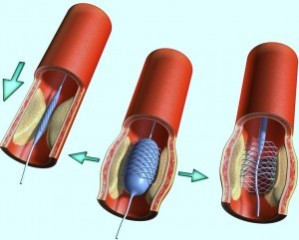
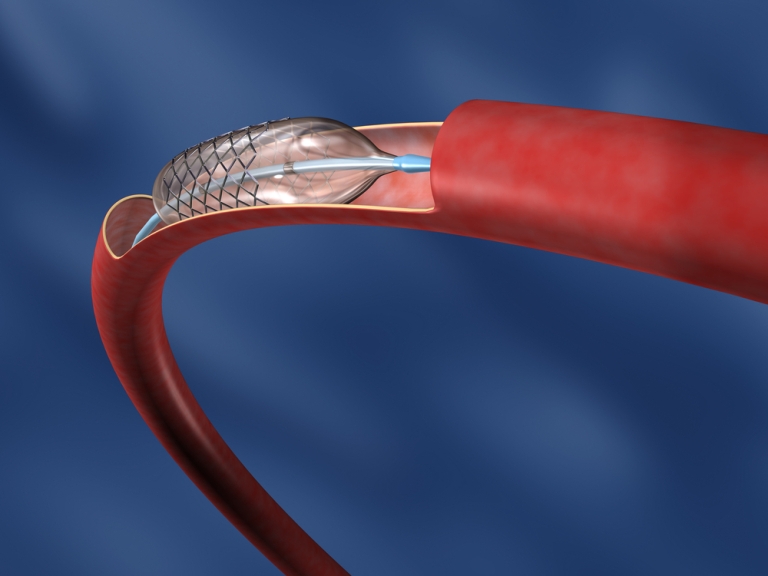
Stenting is an alternative to shunting
 Unlike the procedure for creating an anastomosis from a venous or arterial donor, this operation involves the installation of a stent, which eliminates the narrowing of a metal mesh structure, plain or coated with a drug.
Unlike the procedure for creating an anastomosis from a venous or arterial donor, this operation involves the installation of a stent, which eliminates the narrowing of a metal mesh structure, plain or coated with a drug.
- no extensive incisions (percutaneous coronary intervention);
- less stress on the body;
- short recovery period;
- fewer contraindications and complications compared to the bypass procedure;
- the possibility of performing the operation under local anesthesia.
- the likelihood of thrombus formation in the area of stent installation increases, which can be up to three or four;
- it is difficult to carry out stenting of arteries with a small diameter, when the lumen is narrowed simultaneously in many places or in a large area of the lesion;
- the introduction of a catheter may be accompanied by the formation of a hematoma at the puncture site, perforation of the coronary artery;
- the appearance of severe allergic and chemotactic reactions to the contrast agent is possible;
- in the future, there is a risk of developing a restenotic process with the need for a second operation.
Thus, although the stenting procedure is an effective way to eliminate the narrowing of the coronary arteries, coronary artery bypass grafting is often the first choice.
Preoperative examination and bypass surgery
 Despite the fact that bypass surgery is a standard procedure, preparation for it requires a complete examination of the patient.
Despite the fact that bypass surgery is a standard procedure, preparation for it requires a complete examination of the patient.
- Ultrasound examination of the heart (echocardiography), which allows you to assess the condition of the heart muscle.
- Electrocardiographic study (ECG).
- Chest x-ray, angiography and coronary angiography (X-ray with a contrast agent) - to assess the condition of the heart vessels and visualize the area of narrowing.
- Ultrasound of the vessels of the lower extremities to assess the condition of donor veins.
- Carrying out cardiological stress tests (stress tests).
- Taking the necessary laboratory tests, in which special attention is paid to the level of hemoglobin, platelets, creatinine, the detection of blood clotting disorders.
- most often - with cardiac arrest and the use of a heart-lung system;
- on a beating heart using a "stabilizer".
- minimally invasive access (endoscopic surgery).
The operation is performed within a few hours (3-4 - with cardiac arrest, up to 6 - with a beating heart) under general anesthesia. Surgical intervention performed without cardiac arrest has a number of advantages, such as a reduction in the duration of the operation and the recovery period, a reduction in trauma and the risk of complications. However, in cases of atherosclerotic lesions of several areas (multifocal atherosclerosis) or in the presence of combined cardiopathology, shunting on a beating heart is not performed.
If necessary, the patient is prescribed therapy in advance using antiplatelet agents - drugs that prevent the formation of blood clots. Directly on the day of the operation, it is forbidden to eat, the amount of liquid consumed is sharply limited. Antianginal (stopping angina) means of withdrawal do not require.
Before surgery, premedication with sedatives is performed to reduce anxiety and anxiety.
 The operation itself consists of several stages:
The operation itself consists of several stages:
- Introduction of intravenous anesthesia.
- Insertion of a gastric tube, urinary catheter and endotracheal tube into the trachea for breathing using a mechanical ventilation device (ALV).
- Making a vertical incision along the midline of the sternum to access the heart.
- Collection of a donor vein or artery.
- During surgery on a non-working organ, the patient’s heart stops and is connected to the artificial circulation system.
- Formation of a bypass.
- Restoration of the work of the heart.
- Installing a drain and closing the chest cavity.
After that, the operated patient, until the condition stabilizes, enters the intensive observation unit with connection to the ECG monitor. Appropriate drug treatment is prescribed: antibacterial, analgesic, anti-inflammatory; continued antiplatelet therapy. Then, usually after 1-2 days of strict bed rest, the patient is transferred to a regular room. The sutures are removed on the sixth or seventh day.
After transfer to the cardiac surgery department, in the absence of pathological signs, the patient is allowed to gradually increase physical activity. In order to prevent the development of postoperative complications (infection of the wound, blockage of the shunt, possible bleeding), blood counts are necessarily monitored. To assess the effectiveness of the procedure, the patient is examined using instrumental methods. In order to avoid accumulation of fluid in the lungs and the development of pneumonia, one should not allow immobility, control the change in body position. Breathing exercises are recommended.
Rehabilitation and recovery
 The duration of the patient's stay in the hospital is determined individually and depends on the clinical picture, the presence of complications and the characteristics of the surgical intervention. On average, it does not exceed ten days. In the first week after discharge, patients can return to work, but heavy lifting and physical overexertion should be avoided.
The duration of the patient's stay in the hospital is determined individually and depends on the clinical picture, the presence of complications and the characteristics of the surgical intervention. On average, it does not exceed ten days. In the first week after discharge, patients can return to work, but heavy lifting and physical overexertion should be avoided.
- restoration of blood supply to the heart in full;
- cessation or significant reduction in the number of angina attacks;
- reduction of shortness of breath, pain;
- reducing the risk of myocardial infarction;
- increasing physical endurance and improving the quality of life of the patient.
In the future, patients need to be monitored by a local therapist and monitor the state of the heart for the timely detection of possible complications.
In the near and distant period of time, these can be:- persistent anginal pain, return of angina pectoris;
- the formation of keloid scars;
- cardiac arrhythmia;
- shunt occlusion;
- myocardial infarction;
- hemorrhagic or ischemic stroke, accompanied by a high level of mortality and disability;
- inflammatory process in the tissue of the mediastinum;
- death.
The likelihood of developing serious complications is not very high. As a rule, the factors provoking their development are the patient's advanced age, female gender (due to the smaller diameter of the arteries), the presence of various chronic pathologies: renal failure, hormonal disorders (such as diabetes mellitus), lung diseases, blood clotting disorders.
Forecast and prevention
 Despite the good efficiency of the operation, the installation of shunts only eliminates the consequences of atherosclerotic vascular lesions, but does not eliminate the root cause. The main task of the patient who underwent coronary artery bypass grafting is to review the usual lifestyle, which plays an important role in the predicted future.
Despite the good efficiency of the operation, the installation of shunts only eliminates the consequences of atherosclerotic vascular lesions, but does not eliminate the root cause. The main task of the patient who underwent coronary artery bypass grafting is to review the usual lifestyle, which plays an important role in the predicted future.
- Medical management of arterial hypertension.
- Regular monitoring by a doctor and strict implementation of his recommendations.
- Refusal of smoking and strong alcohol.
- Treatment with statins to lower cholesterol levels.
- In the presence of diabetes - compensation for the disease, taking hypoglycemic drugs.
- Daily outdoor physical activity.
- Use of compression underwear.
- Body weight control.
- Annual spa treatment.
- Reducing stress to a minimum.
- Seasonal influenza vaccination to reduce the risk of worsening coronary heart disease during an epidemic.
- Dieting.
- the exclusion of fried and fatty foods, white flour bakery products, sweet muffins, carbonated drinks, strong tea and coffee, fast food;
- replacing meat products (in particular, pork and duck) with fish, and sweets and sugar with honey and dried fruits;
- strict restriction of the amount of salt consumed (daily norm - half a teaspoon);
- replacement of animal fats with olive oil;
- taking as a basis for the diet the use of boiled beef, sour-milk and low-fat dairy products, liver, buckwheat, oatmeal, seasonal vegetables and fruits, walnuts, almonds, greens (spinach is especially useful).
 Reducing the risk of relapses, as well as curbing the pathological process, can only be achieved by a set of therapeutic and preventive measures. It is important to understand that only complete restoration and strengthening of the body leads to recovery and improves the long-term prognosis.
Reducing the risk of relapses, as well as curbing the pathological process, can only be achieved by a set of therapeutic and preventive measures. It is important to understand that only complete restoration and strengthening of the body leads to recovery and improves the long-term prognosis.
The average life expectancy after coronary bypass surgery is 15 to 18 years. Almost half of the patients overcome the twenty-year milestone. Thirty-year survival among patients reaches 15%.
That is why, at the end of the article, we give feedback from patients who underwent this operation with good results:
Discharged from the hospital on the seventh day. If it weren't for the temperature, we probably could have been on the fifth. There was no pain, but a mountain of antibiotics was prescribed, to which he reacted with itching, diarrhea, and the like. At first it was difficult to breathe at night, because of this, the first couple of weeks I had to sleep half-sitting. For about a month there was weakness, he could barely crawl, then gradually it got better. The doctors said that it was necessary to immediately give physical activity, so every day I paced with all my might and tried not to lie too long. And since the chest pain disappeared immediately and forever, it was very uplifting.
It costs 3 shunts and 1 stent. The first two or three days were very difficult, but the doctor said that in two months the operation would be forgotten like a bad dream. It gives strength. Now a month and three days have passed. There is no pain, but the seam is very itchy. Before the operation, he did not part with nitroglycerin at all, but now he has completely abandoned it. Before being discharged, they were forced to take a test. The result is 45 steps per minute.
Before the operation, I did not know the way to the garden. Breakfast, second breakfast, lunch (1st, 2nd and compote), rest! And so on. After the operation, I “jump” from the cultivator to the lawn mower, and I also water it in the greenhouse.
Survived this difficult operation, 62 years old. Previously, she could hardly walk, she suffered from shortness of breath. Now I feel great, I even began to sing in the choir. But I had no other serious illnesses that forbade surgery.
I am 53 years old. He underwent the operation easily, only the lungs were expectorated for a long time. It's been 3 months. I ski for 5 km without problems, to the 5th floor without stopping. After the operation, only the sternum hurt - no coughing, no sneezing. The rest is all good. The pulse became 60, and was 80. And the pressure at rest was 120 to 80. I measured it after skiing - 130 to 90. So this is salvation. 4 vessels were clogged - one at 100 percent, three at 80 percent. The heart attack was behind him. And there's nothing to be afraid of. He closed his eyes, opened them, and after 5 days he was in his hospital. And there in 10 days home. A month later I went to work, however, physically did nothing.
My dad had surgery 7 years ago at 60. On the third day, he was transferred from the intensive care unit to the department. I immediately tried to get up. Due to the fact that the vein was taken from the leg, it was necessary to move so that the blood would not stagnate. I ate a little, after which I had the strength to get up on my own to go to the toilet. There was a temperature. The father was discharged five days later. I went to a sanatorium, where I came to my senses a little, and finally recovered at home. The difficulties were not so much physical as psychological. My sternum was still very sore, and for several years afterwards it was painful to cough. He went to work two months later. Now he annually does coronary angiography. Age-related sores have already climbed, but everything is fine with the heart. Continues to work hard. Drinks medicine.
Three years ago, I underwent CABG (four shunts were placed on a beating heart), and six months later they cleaned my carotid artery. They did not dare to do two operations at the same time. I gave up smoking 10 months before the operation. I have not drunk alcohol for many years. Today (in three months I should be 70 years old) I feel quite comfortable! I went to the operation with a philosophical approach: if I don’t wake up after anesthesia, then I still won’t know about it. But how much time the Lord will let me go now, probably only he knows. Personally, I determined my life qualification at 128 years old! As they say, if you want a hundred, ask for two hundred!
I had 2 heart attacks 11 years ago. Angina pectoris was terrible, without nitroglycerin he could not even take two steps. And 10 years ago they did CABG, 3 shunts. The quality of life has improved by 95%. Fishing, mushrooms, a beloved woman, a glass of tea, a dacha - these pleasures were not there before the operation. If there is an indication for shunting, do not hesitate. The stenoses are increasing, and the toothless with a scythe will not linger. I wish you success.